
Anatomy
| Number | Name | Sensory, | Origin | Nuclei | Function |
|---|---|---|---|---|---|
| 0 | Cranial nerve zero (CN0 is not traditionally recognized.) | Sensory | olfactory trigone, medial olfactory gyrus, and lamina terminalis | New research indicates CN0 may play a role in the detection of pheromones Linked to olfactory system in human embryos | |
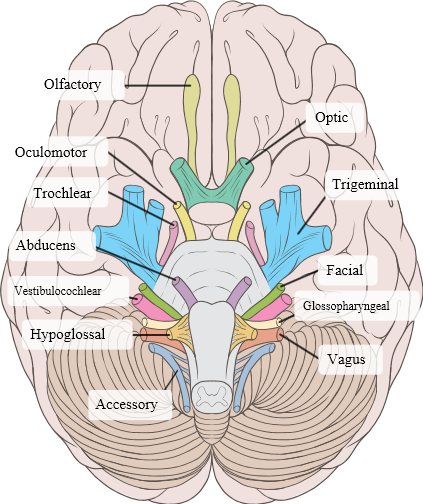
| I | Olfactory nerve | Purely Sensory | Telencephalon | Anterior olfactory nucleus | Transmits the sense of smell; Located in olfactory foramina in the Cribriform plate of ethmoid |
| II | Optic nerve | Purely Sensory | Diencephalon | Ganglion cells of retina | Transmits visual information to the brain; Located in optic canal |
| III | Oculomotor nerve | Mainly Motor | Anterior aspect of Midbrain | Oculomotor nucleus, Edinger-Westphal nucleus | Innervates levator palpebrae superioris, superior rectus, medial rectus, inferior rectus, and inferior oblique, which collectively perform most eye movements; Also innervates m. sphincter pupillae, as well as the muscles of the ciliary body. Located in superior orbital fissure |
| IV | Trochlear nerve | Mainly Motor | Dorsal aspect of Midbrain | Trochlear nucleus | Innervates the superior oblique muscle, which depresses, rotates laterally (around the optic axis), and intorts the eyeball; Located in superior orbital fissure |
| V | Trigeminal nerve | Both Sensory and Motor | Pons | Principal sensory trigeminal nucleus, Spinal trigeminal nucleus, Mesencephalic trigeminal nucleus, Trigeminal motor nucleus | Receives sensation from the face and innervates the muscles of mastication; Located in superior orbital fissure (ophthalmic nerve - V1), foramen rotundum (maxillary nerve - V2), and foramen ovale (mandibular nerve - V3) |
| VI | Abducens nerve | Mainly Motor | Posterior margin of Pons | Abducens nucleus | Innervates the lateral rectus, which abducts the eye; Located in superior orbital fissure |
| VII | Facial nerve | Both Sensory and Motor | Pons (cerebellopontine angle) above olive | Facial nucleus, Solitary nucleus, Superior salivary nucleus | Provides motor innervation to the muscles of facial expression, posterior belly of the digastric muscle, and stapedius muscle, receives the special sense of taste from the anterior 2/3 of the tongue, and provides secretomotor innervation to the salivary glands (except parotid) and the lacrimal gland; Located and runs through internal acoustic canal to facial canal and exits at stylomastoid foramen |
| VIII | Vestibulocochlear nerve (or auditory-vestibular nerve or statoacoustic nerve) | Mostly sensory | Lateral to CN VII (cerebellopontine angle) | Vestibular nuclei, Cochlear nuclei | Senses sound, rotation and gravity (essential for balance & movement). More specifically. the vestibular branch carries impulses for equilibrium and the cochlear branch carries impulses for hearing.; Located in internal acoustic canal |
| IX | Glossopharyngeal nerve | Both Sensory and Motor | Medulla | Nucleus ambiguus, Inferior salivary nucleus, Solitary nucleus | Receives taste from the posterior 1/3 of the tongue, provides secretomotor innervation to the parotid gland, and provides motor innervation to the stylopharyngeus. Some sensation is also relayed to the brain from the palatine tonsils. Sensation is relayed to opposite thalamus and some hypothalamic nuclei. Located in jugular foramen |
| X | Vagus nerve | Both Sensory and Motor | Posterolateral sulcus of Medulla | Nucleus ambiguus, Dorsal motor vagal nucleus, Solitary nucleus | Supplies branchiomotor innervation to most laryngeal and all pharyngeal muscles (except the stylopharyngeus, which is innervated by the glossopharyngeal); provides parasympathetic fibers to nearly all thoracic and abdominal viscera down to the splenic flexure; and receives the special sense of taste from the epiglottis. A major function: controls muscles for voice and resonance and the soft palate. Symptoms of damage: dysphagia (swallowing problems), velopharyngeal insufficiency. Located in jugular foramen |
| XI | Accessory nerve (or cranial accessory nerve or spinal accessory nerve) | Mainly Motor | Cranial and Spinal Roots | Nucleus ambiguus, Spinal accessory nucleus | Controls sternocleidomastoid and trapezius muscles, overlaps with functions of the vagus. Examples of symptoms of damage: inability to shrug, weak head movement; Located in jugular foramen |
| XII | Hypoglossal nerve | Mainly Motor | Medulla | Hypoglossal nucleus | Provides motor innervation to the muscles of the tongue (except for the palatoglossus, which is innervated by the vagus) and other glossal muscles. Important for swallowing (bolus formation) and speech articulation. Located in hypoglossal canal |
Assessment
| Nerve | Evaluation | Associated Conditions |
|---|---|---|
| I: Olfactory Nerve | - Smell is tested in each nostril separately by placing stimuli under one nostril and occluding the opposing nostril. - The stimuli used should be non-irritating and identifiable. eg cinnamon, cloves and toothpaste. - Bilateral loss can occur with rhinitis, smoking or aging. - Unilateral loss indicates a possible nerve lesion or deviated septum. - This test is usually skipped on a cranial nerve exam. | Meningioma |
| II: Optic Nerve | - Visual acuity is tested in each eye separately. - Ensure the patient’s vision is corrected with eyeglasses or a pinhole. The patient is asked to read progressively smaller lines on the near card or snelen chart. - Visual fields are assessed by asking the patient to cover one eye while the examiner tests the opposite eye. The examiner wiggles the finger in each of the four quadrants and asks the patient to state when the finger is seen in the periphery. The examiner’s visual fields should be normal, since it is used as the baseline. - Pupillary light reflex - The patient stares into the distance as the examiner shines the penlight obliquely into each pupil. Pupillary constriction should be noted on the eye examined (direct response) and on the opposite eye (consensual response). The swinging flashlight test involves moving the light between the two pupils. Normally both direct and consensual responses are ellicited when the light shines on an eye, and some dilation will occur during the swing between. | |
| III, IV, VI: Oculomotor nerve, Trochlear nerve, Abducens nerve | Extraocular movements - First, inspect for ptosis, eye position and nystagmus. - The pupil size should be measured, its shape and any asymmetry should be noted. A commonly used abbreviation to describe normal pupils is PERRLA (pupils equal, round and reactive to light and accommodation). - The examiner tests ocular movements by standing one meter in front of the patient and asking the patient to follow a target with eyes only, and not the head. The targets is moved in an “H” shape and the patient is asked to report any diplopia. Then, the target is held at the lateral ends of the patient’s visual field. Nystagmus should be noted. One or two beats is a normal finding. - The accommodation reflex is tested by moving the target towards the patient’s nose. As the eyes converge, the pupils should constrict. - The optokinetic nystagmus test is optional and involves asking the patient to look at a moving strip of horizontal lines. Nystagmus is normally observed. | |
| V: Trigeminal nerve | Sensation - Light touch is tested in each of the three divisions of the trigeminal nerve and on each side of the face using a cotton wisp or tissue paper. - The ophthalmic division is tested by touching the forehead, the maxillary division is tested by touching the cheeks, and the mandibular division is tested by touching the chin. Be careful not to test the mandibular division too laterally, as the mandible is innervated by the great auricular nerve (C2 and C3). A common mistake is to use a stroking motion, which will trigger pain and temperature nerves. Instead, a point stimulus should be applied. - For pain and temperature repeat the same steps as light touch but use a sharp object and a cold tuning fork respectively. - Corneal reflex is conducted along with the facial nerve section of the test. Note the sensory innervation of the cornea is provided by the trigeminal nerve while the motor innervation for blinking the eye is provided by the facial nerve. Motor - Muscles of mastication (temporalis, masseter) should be inspected for atrophy. Palpate the temporalis and masseter as the patient clenches the jaw. The pterygoids can be tested by asking the patient to keep the mouth open against resistance, and move from side to side against resistance. - A jaw jerk reflex can be tested by placing a finger over the patient’s chin and then tapping the finger with a reflex hammer. Normally the jaw moves minimally. | |
| VII: Facial nerve | Inspect for facial asymmetry and involuntary movements. Motor 1) Raise both eyebrows 2) Frown 3) Close both eyes tightly so that you can not open them. Test muscular strength by trying to open them 4) Show both upper and lower teeth 5) Smile 6) Puff out both cheeks Sensory : test for taste | |
| VIII: Vestibulocochlear | Hearing: Whisper numbers in one ear and ask the patient to repeat the numbers. Make sure to cover the opposite ear. Conduct the Rinne test and Weber test. - Vestibular Function | Acoustic Neuroma |
| IX and X: Glossopharyngeal and Vagus | - Gag response - Palatal articulation “KA” - Guttural articulation “GO” | Lateral medullary syndrome (IX) |
| XI: Accessory Nerve | - Shrug shoulders - Turn head from side to side | |
| XII: Hypoglossal | - Inspect for tongue atrophy, fasciculations or asymmetry |